| Lyme Disease and Mental Illness
This article is a work in progress. It is not
complete. Please send any
comments or questions.
 Microbes are the greatest predator of man. As medical technology improves, there is increasing recognition that infectious disease contributes not only to acute, but also chronic relapsing illness and mental illness.
-Robert
C. Bransfield, M.D. Microbes are the greatest predator of man. As medical technology improves, there is increasing recognition that infectious disease contributes not only to acute, but also chronic relapsing illness and mental illness.
-Robert
C. Bransfield, M.D.
Probably the biggest challenge facing those sick
with Lyme disease manifesting with psychiatric symptoms is to get the
Lyme disease diagnosis in the first place. Many people with Lyme and
associated mental dysfunction (this is about 95% of all Lyme sufferers)
never get diagnosed properly and are left to struggle with palliative
treatment, institutionalization, and basically a life sentence of
obscurity and panic.
Even for those with the right diagnosis, for
example, Lyme disease infection, symptoms of mental illness are
obviously still devastating. I created this video to address some of the
common experiences, and some useful solutions / tips, for people who
meet this description. Below the video is an excerpt from a book I wrote
in 2007 entitled The
Lyme-Autism Connection, which further addresses the topic of the
connection between Lyme disease and mental illness.
Excerpt: Mental Illnesses and
Autism, Lyme Disease
From the book, The
Lyme Autism Connection
Symptom similarities between Lyme disease and autism, especially in children, are astounding. Obviously, symptom similarity alone is not a strong enough scientific indicator to implicate Lyme disease in the autism epidemic. However, when considered within the framework of the other arguments presented in this book, symptom similarity becomes an important, central piece of the puzzle.
This chapter was written with three primary goals. First, we will look at the diagnostic procedures used in classifying mental illnesses. Then we will show that a Lyme disease diagnosis overlaps with numerous other mental disorders. Finally, we will show that an autism diagnosis not only overlaps with a variety of different mental illnesses as well, but that they happen to be, in many cases, the same mental illnesses which overlap with Lyme disease. Additionally, the chapter will also cover various data which support the above three points.
Symptoms vs. Syndromes
At first glance, the obvious question to ask in this chapter is whether or not the symptoms of Lyme disease overlap with the symptoms of autism. As you will see, however, this question is much too broad. You will see that Lyme disease is known as the “great imitator” because it can mimic dozens of seemingly unrelated health problems. Lyme disease symptoms overlap with just about every mental illness, so it is not very impressive to show that they also overlap with autism.
For this reason, we will instead take a narrower look at the symptom similarities between Lyme disease and autism, and delve further into analyzing the overlap. Namely, we will not look at individual symptoms the diseases share in common, but instead at entire disease syndromes which the two diseases share in common. For example, we will go further than to just say “Lyme disease and autism both cause headaches.” Rather, we will say that “Lyme disease and autism both manifest as schizophrenia.” A headache is an individual symptom, while schizophrenia is a complex syndrome.
For our purpose of further analyzing the Lyme-autism connection, it is more helpful to look at overlapping disease syndromes instead of just overlapping symptoms because disease syndromes are much more complex, specific, and isolated than are individual symptoms. Many things can cause a headache, such as fatigue, a bad lunch, or a fight with a spouse. So, demonstrating that Lyme disease and autism both cause headaches does not add much support to the Lyme-autism connection. Schizophrenia, on the other hand, is not caused by many factors, and cannot be confused with simple triggers like a bad hamburger or emotional stress. By narrowing the comparison down to specific disease syndromes, we can build a much stronger case for the Lyme-autism connection.
Blurred Lines Between Disease Labels
In order to show that both Lyme disease and autism share in common numerous disease syndromes, we must first accept the fact that the diagnostic lines are blurred between autism, Lyme disease, and numerous other mental illnesses, leading to somewhat arbitrary and meaningless guidelines for diagnosing the diseases. For example, someone diagnosed with the label “schizophrenia” may in fact be suffering from Lyme disease, autism, or both. “Schizophrenia” is not a disease; instead it is a disease presentation. The label schizophrenia says nothing about the reason for the disease, or the cause, but instead simply says that a given person is suffering from a collection of physiologic and symptomatic dysfunctions.
It is important to keep this in mind as you think about Lyme disease, autism, and the list of mimicking diseases. You have to ask yourself, “Does the disease label in question tell me anything about what is actually causing this health problem?” Understanding that many of the disease labels used by conventional medicine are actually not indicative of the cause of the disease will help you learn how to adjust your thinking process and see that many “diseases” do not in fact have established, defined boundaries separating them from other “diseases,” but are instead simply a melting pot of symptomatic and physiological characteristics.
Why is this important? Let’s again use the example of a headache. When someone says, “I have a headache,” you would never jump to a conclusion about what is causing the headache unless you knew more about the person’s current circumstances. A headache is not a disease in and of itself; instead it is a list of symptomatic and physiologic properties, namely, pain in the head, and typically, inflammation in the head. We all know that many things can cause headaches, hence, if someone mentions their headache, the next thing you might try to do is play detective to discover what is causing the headache. You might ask the person what they ate for lunch, how much sleep they are getting, or what is happening at work. You would never assume that the cause of their headache is the headache itself. Headaches always have underlying, root causes.
In the same way, if someone has schizophrenia or autism, you should train your mind to play the same detective role. Schizophrenia and autism are no more the cause of a health problem than is a headache. Instead, schizophrenia and autism are just labels for a set of symptomatic and physiologic characteristics. When you begin to adopt this way of thinking, you can see that the lines between various diseases can easily become blurred.
When autism is seen as a set of symptoms rather than a defined “disease,” it leaves a lot more room for questions—questions which can ultimately lead to a better understanding of the disease and its cause(s). Do not passively accept a diagnosis of autism as the final description of your child’s health. You should empower yourself to play detective and get to the bottom of the symptoms, instead of simply accepting the diagnosis and giving up.
If you think about Lyme disease and autism as separate diseases, with distinct boundaries, then the Lyme-autism connection seems improbable. However, if you think of the two diseases accurately, as nothing more than arbitrary labels which encompass a grouping of symptoms, some of which overlap, then the question arises and must be answered: what is the root cause of the disease syndromes? Is the root cause potentially the same?
Now, a clarifying point is in order here. Some diseases certainly do include causative factors in their label. For example, strep throat is caused by…strep bacteria in the throat. The disease label “strep throat” is one which is accurate in its description of causality. Similarly, Lyme disease is caused by Lyme disease bacteria (the scientific name for which is Borrelia burgdorferi). So, when we are looking at the Lyme-autism connection, what we are really asking is whether or not autism shares the same root cause as Lyme disease, namely, a Borrelia infection.
Ok, so this all sounds good in theory, but where is the evidence? Let’s now turn our attention to several scientific studies which provide objective substantiation for the theory we just talked about—the theory that mental disorders have blurred diagnostic lines.
Lyme Disease: The Great Imitator
To substantiate the theory that disease labels are relatively arbitrary and have blurred defining lines, let’s begin by looking at Lyme disease and the many diseases which it mimics.
The Journal of Neuropsychiatry in 2001 published an article in which it was stated that “Children with Lyme disease have…cognitive and psychiatric disturbances…resulting in psycho-social and academic impairments.” According to Dr. Frederic Blanc, of the University of Strasbourg, France, “The neurological and psychiatric manifestations of Borrelia are so numerous that it is called the ‘new great imitator.’ Every part of the nervous system can be involved: from central to peripheral.”
It is difficult to convey just how broad and diverse Lyme disease symptoms can be. As the “new great imitator” (Syphilis was considered the original great imitator), Lyme disease mimics dozens of seemingly unrelated illnesses, from physical disorders such as chronic fatigue syndrome and arthritis, to psychiatric disorders including schizophrenia, obsessive compulsive disorder, Tourette syndrome, depression, bipolar disorder, and more. According to psychiatrists at Columbia University, as published in 1994 in the American Journal of Psychiatry:
“Lyme disease can trigger a broad range of psychiatric reactions, including paranoia, dementia, schizophrenia, bipolar disorder, panic attacks, major depression, anorexia nervosa and obsessive–compulsive disorder.”
As you can see, Lyme disease is often the root cause of a long list of diseases. In these cases, there is in fact zero separation between the seemingly distinct diseases on the list—the lines are blurred beyond recognition. A variety of mental disorders can potentially all have the same root cause.
Antiquated belief that Lyme disease is characterized by a limited set of mostly benign symptoms is rapidly being replaced by modern, increasingly accurate models of Lyme disease symptomology that encompass a vast diversity of symptomology in numerous body systems. So, if you are doubtful that a simple bacterial infection can cause such diverse symptoms as are present in autism, be forewarned—Lyme disease is a highly advanced neuropsychiatric disease with complicated and poorly understood effects on the brain. The combination of wide-ranging symptoms and the prevalence of false-negative laboratory test results means that Lyme disease may be one of the most rampant, yet under-diagnosed, infections on the planet. And, when the Lyme infection occurs in the womb, a new set of variables and complexities are introduced to the scene which further broaden the potential neurological effects of Lyme disease.
Still, the fact that Lyme disease is a great imitator is nothing worth writing home about—this has become accepted science in both mainstream and alternative medicine. Therefore, we will not belabor this point here. To learn more about Lyme disease as a great imitator, read Appendix B and consult available Lyme disease literature.
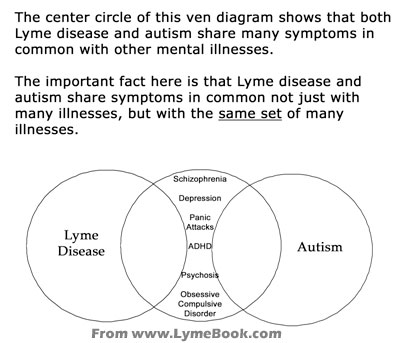
The real point we are tracking down in this chapter is not merely the fact that Lyme disease shares blurred lines with many mental illnesses, but, more importantly, the fact that autism also shares blurred lines with a variety of mental disorders. Even more important yet is the paramount question of whether or not Lyme disease and autism share blurred lines with the same set of mental illnesses.
Autism: The Next Great Imitator?
You may be surprised to learn that just as Lyme disease is a great imitator, so also is autism.
Many autistic people have a broad range of psychological symptoms, not just those few which have historically defined “classic” autism. Autism is currently being re-defined as a multi-systemic, multi-factorial disease. In this section, we will examine some of the science surrounding autism as a great imitator. For each of the scientific studies below, we will note their relevance to the Lyme-autism connection.
Swedish researchers have observed a fascinating overlap between symptoms of autism and other mental illnesses. In 2004, the Department of Child and Adolescent Psychiatry, at Göteborg University, Sweden, published findings in the Journal of Neural Transmission indicating that patients suffering from autism also sometimes have symptoms of schizophrenia, bipolar disorder, and attention-deficit/hyperactivity disorder (AD/HD). The Swedish researchers don’t offer an explanation for this symptom overlap, but they do acknowledge it, and conclude their study by stating that “Current diagnostic criteria have to be revised to acknowledge the co-morbidity of autism with bipolar disorder, AD/HD, schizophrenia, and other psychotic diseases.”
The connection: Of the mental illnesses which Lyme disease mimics, schizophrenia, bipolar disorder, and attention-deficit/hyperactivity disorder are at the top of the list.
Researchers at the University of Michigan published a study in 2004 in the Journal of Autism and Developmental Disorders which concluded with the following statement: “This study lends support to the validity of depression as a distinct condition in some children with autism/PDD and suggests that, as in the normal population, autistic children who suffer from depression are more likely to have a family history of depression.”
The connection: These findings are significant for two reasons: first, the study indicates that depression is part of the autism complex of symptoms, and second, this depression can be found in family history. Both of these points are true of Lyme disease, as well.
In London, similar conclusions are being reached. The Genetic and Developmental Psychiatry Research Centre published in 1998 a study entitled “Autism, affective and other psychiatric disorders: patterns of familial aggregation.” The report was released by Cambridge University Press in the Journal of Psychological Medicine. In addition to finding a correlation between familial mental disorders and autism, researchers also discovered that “Individuals with a singular diagnosis of obsessive-compulsive disorder were more likely to exhibit autistic-like social and communication impairments.”
The connection: This finding is fascinating because it tells us that not only does autism involve symptoms of other, previously believed separate diseases, but the converse of this is also true; that those separate diseases also sometimes include symptoms known to occur in autism. This further blurs the lines between different mental disorders. This is another piece of the puzzle that shatters the previous belief that autism is completely distinct and separate from other psychiatric diseases. Modern medicine likes to put these diseases in their own neatly organized, unrelated files, but reality just won’t comply with such an organizational strategy.
City of Hope National Medical Center in California published findings that link autism and Tourette syndrome. Researchers found that “there is an intimate genetic, neuropathologic relatedness between some cases of [autism] and Tourette syndrome.” Additionally, these researchers noted frequent family groupings of the two afflictions, with obsessive compulsive disorder also showing up frequently.
The connection: The Lancet in 1998 published a study linking Lyme disease with Tourette syndrome. A 4-year old boy developed typical Tourette symptoms and was subsequently diagnosed with Lyme disease by ELISA IgG antibody testing. Upon antibiotic treatment, all symptoms resolved. From the Lancet: “Rapid efficacy of antibiotic treatment followed by a decrease in Borrelia-specific antibody titres suggests that the multiple motor and vocal tics [in this 4-year old boy] were at least partially caused by the tertiary stage of Borreliosis.” Therefore, both autism and Lyme disease share in common blurred lines with Tourette syndrome.
The lines between autism and other mental disorders are further blurred when considering the methods used to diagnose autism. This is an important area to examine because the diagnostic model used in categorizing childhood mental disorders is the primary determinant of the next twenty or more years of treatment decisions. Consider this carefully—if a child is diagnosed with autism but Lyme disease is really the root problem, then parents will spend thousands (or maybe millions) of dollars, thousands of hours, and incalculable stress, pursuing the wrong course(s) of treatment. Hence, proper diagnostic procedures, or at least, proper understanding of the limitations of modern diagnostic capabilities, is essential for ensuring that a lifetime of energy is focused in the right direction. This statement is substantiated by the experiences of numerous mothers, whose stories appear in Appendix E. These mothers only received desirable treatment results after discovering the Lyme infection in their children. Prior to the discovery, they wasted incalculable time, energy and money chasing palliative treatments.
Alarmingly, the diagnostic model used for autism can be relatively unreliable. The Indiana University School of Medicine in 1971 evaluated 5 diagnostic systems designed to differentiate infantile autism and early childhood schizophrenia and published their findings in the Journal of Autism and Developmental Disorders. Diagnostic scores from 44 children were examined. Some of the five diagnostic systems contradicted the others, leading to a confusing and disturbing debate about the definitions of autism and schizophrenia. So similar are the two diseases that the lines between them become blurred when using these diagnostic systems, and the results of the diagnostic procedures become relatively meaningless. Obviously, diagnostic systems have improved exponentially since 1971. However, even today, the same symptom similarities exist between autism and schizophrenia, resulting in debate and disagreement about proper courses of treatment for the two disorders, not to mention heated arguments between parents and physicians about which treatments are most logical to pursue. Modern medicine’s appearance of having everything figured out, with white-coated, authoritative doctors passing down final diagnostic decrees to parents, is riddled with an uncertain and ambiguous past.
The tendency to over-compartmentalize diseases without sufficient data is not limited to just the commercial medical industry—non-profit research organizations dedicated to healing schizophrenia and autism also suffer the effects of arbitrarily separating autism from schizophrenia when conducting research and presenting information. The reality is that autism and schizophrenia are intimately related, and only when this fact is accounted for will true breakthrough occur in the research of the two conditions. Autism and schizophrenia are not two separate entities like the colors black and white. They resemble more closely a shade of grey, mixing some amount of black and some amount of white. When researchers only look at the black, they miss the big picture, and when they only look at white, they don’t see all of the facts. Only when shades of grey are acknowledged, will the mechanisms behind the afflictions become more apparent.
Any parent with an autistic child knows that their child exhibits a wide array of symptoms and that no two days are alike. Unlike high cholesterol or diabetes, which are fairly constant disorders with very few variations in symptoms and presentation, autism is a wildly variable condition that seems to follow no particular pattern or predictable course.
Thus far in this chapter, we have worked to establish that not only do Lyme disease and autism act like great imitators, but the diseases which they imitate happen to be the same diseases—namely, mental disorders such as schizophrenia, obsessive compulsive disorder, depression, Tourette syndrome, AD/HD, and others. Although this overlap in associated disease syndromes (and, more broadly, associated individual symptoms) is not sufficient evidence to stand alone as the foundation for the Lyme-autism connection, this observation is, again, one more piece of the puzzle.
It really is shocking and insightful to discover that Lyme disease and autism are separated by much less space than medical schools and textbooks teach. If these broad similarities are not explained by an underlying Lyme disease infection, then what is the explanation? Isn’t it a bit improbable that two supposedly separate diseases are so intimately related in so many ways?
Before concluding this chapter, we will briefly introduce one more area of overlap: autoimmunity.
Autoimmunity
Lyme disease and autism not only share numerous similarities with regard to psychiatric symptoms and syndromes, but also autoimmunity.
The number of studies linking both Lyme disease and autism to autoimmune dysfunction is vast, encompassing dozens of published articles released by several research institutions. For specific studies, visit MEDLINE at www.ncbi.nlm.nih.gov/PubMed and search for keywords autism autoimmune and lyme disease autoimmune. At the time of this writing, the first search string yielded 86 studies and the second string yielded 123 studies.
The fact that Lyme disease and autism share autoimmunity in common is, of course, fascinating, and lends credit to the Lyme-autism hypothesis. However, the link becomes even stronger in light of the fact that new research is revealing that many autoimmune disorders are caused by stealth infections. Recent research has found that treatments aimed at eradicating stealth infections happen to also provide relief, and in some cases, remission or cure, for autoimmune diseases.
One such cutting-edge treatment is the Marshall Protocol, discussed at length in The Top 10 Lyme Disease Treatments. The Marshall Protocol is significant in this context because it defines and reveals the mechanism by which symptoms of autoimmunity can really be an indication of underlying infection. Patients experiencing healing on the Marshall Protocol suffer from a wide range of autoimmune disorders—and healing is taking place via the anti-infective treatments that comprise the protocol. Autoimmunity is defined as the body attacking its own cells. But why would it do that? The new, prevailing theory is that there is a stealth infection inhabiting body tissues and when the immune system attempts to attack that infection, it mistakenly attacks its own proteins which might look similar to the proteins that compose the infectious microorganisms. This new theory of autoimmunity is gaining momentum.
It shouldn’t surprise us that autoimmunity is involved in Lyme disease. After all, Lyme disease is known to be caused by an infection. However, what about autism? Why is there autoimmunity in autism? Is there an underlying infection? If, in fact, autoimmunity is caused by an infectious process, then the autoimmune link between Lyme disease and autism becomes quite telling and is, yet again, just another piece of the puzzle.
Where the Rubber Meets the Road
Hopefully, this chapter has given you a new perspective on childhood developmental disorders. Remember, if your child gets diagnosed with any of the disease labels we have just looked at, do not be satisfied with the diagnosis. Being diagnosed with attention deficit disorder is like being diagnosed with a headache. A headache is not a diagnosis, it is a symptom. A headache is the beginning of the diagnostic journey, not the end. The same can be said of attention deficit disorder.
The minute you start treating your child’s attention deficit disorder (or autism, or schizophrenia, or fill-in-the-blank disorder) as if it is a complete diagnosis, you are beginning a losing battle. Why? The reason is logical and simple. Since these disease labels do not factor in the true cause(s) of the disease (whatever the cause(s) may be), the only treatment modern medicine can offer you is palliative treatment. Palliative treatment is that which covers symptoms instead of addressing cause. The word palliative is derived from the Latin word palliare, which means “to cloak.”
Antidepressant drugs are an example of a palliative treatment, and, not surprisingly, antidepressant drugs are the treatment most often given for childhood developmental disorders. Other palliative drugs include anti-psychotic, anti-anxiety, and sedative. These drugs only temporarily snuff out the symptoms of the underlying problem. And, these drugs have ghastly, brutal side effects of which the public is becoming increasingly aware—such as aggressive behavior, suicidal thoughts and ideation, and decline in intellect. Are these horrendous side effects justified given that the drugs are not even addressing the cause of the disease?
Most of the autism treatment programs and centers in the United States (at least among mainstream medicine) do nothing but offer palliative, or “behavioral” treatment. The government, non-profit research organizations, and parents spend millions of dollars on palliative treatments for childhood developmental disorders. What would happen if some of that money were actually spent on what really matters; that is, trying to locate and treat the cause? Would you offer physical therapy to someone suffering from a broken leg, or would you repair the broken leg?
Now that you are equipped with knowledge, and you know that childhood developmental disorders do in fact have underlying, scientific, physiological causes (even though these causes are sometimes elusive and difficult to isolate), you can begin to play detective with your child and treat the causes, not the symptoms, of their disease. Palliative treatments are useful to increase quality of life during the discovery process. But the palliative treatments themselves are not the end goal.
Maybe your child’s disorder is caused by an imbalance of intestinal microflora. In this case, you might consider using probiotics, diet, and herbs to correct the problem. Or maybe, it is mercury poisoning, for which you could use chelation. Or possibly, your child’s disorder is caused by food allergies, which you might alleviate by an elimination diet. Or, as this book proposes, maybe your child’s autism is caused by Lyme disease, in which case you may decide to undergo Lyme treatment. Whatever the underlying cause, the thought pattern is the same: you, as the parent, must step up to the plate, take responsibility, reject the “diagnosis” your child was given, and search for the underlying cause.
A good friend of mine (Bryan) suffered from migraine headaches for years. She drained her bank account trying the strongest painkillers and anti-migraine medications available. She endured the side effects of powerful, dangerous pharmaceuticals. She only received minimal relief, and suffered greatly. One day, a thinking physician inquired about her diet and discovered that she consumed diet soda pop once or twice a day, every day of her life. In fact, if she ran out of soda, she would make a special trip to the store to replenish her stock. After she objected vehemently, he finally convinced her to go without the soda for a few weeks. Bingo! The headaches disappeared, almost overnight. The palliative, symptom-covering painkillers were not the answer (although they did make a few CEOs and stockholders richer). Eliminating the root cause was the answer.
I do not want to oversimplify childhood developmental disorders. In most cases, the detective work necessary is much more difficult than the experience my friend had with her headaches. However, you owe it to yourself and your child to at least try the detective strategy. In the best case scenario, you will cure your child, and in the worst case scenario, you will at least become educated about your son or daughter’s body, and provide him or her with some level of relief, however minor. But most importantly, taking a detective approach will ensure that you are doing absolutely everything you can to be a good parent.
You, as a thinking, caring, intelligent parent, have what it takes to be a detective and to reject the superficial diagnosis given by a doctor whose thinking is victim of the dogmatic, palliative treatment paradigm that currently rules American medicine.
|